Quick Facts
- Prevalence: Approximately 1 in 6 adults in the United States report experiencing dysphagia, though only about half discuss it with a clinician.
- Etymology: The term comes from the Greek 'dys' (difficulty) and 'phagia' (to eat).
- Anatomy: The esophageal wall consists of four distinct layers: the mucosa, submucosa, muscularis propria, and adventitia.
- Muscle Composition: The esophagus transitions from entirely striated muscle in the upper third to entirely smooth muscle in the lower third.
- Mortality Risk: Roughly 60,000 deaths occur annually due to complications such as aspiration pneumonia.
- Primary Diagnostic Tool: Upper endoscopy is the gold standard for identifying structural obstructions or inflammation.
Dysphagia swallowing difficulty is more than just a minor annoyance; it is a clinical condition affecting millions of people. Understanding the esophageal anatomy and swallowing function is the first step toward diagnosis. Esophageal dysphagia occurs when food or liquid feels stuck in the throat or chest after swallowing has begun. This condition is distinct from oropharyngeal dysphagia, which involves difficulty initiating a swallow or moving food from the mouth to the throat. Common causes of esophageal issues include esophageal strictures, inflammation from gastroesophageal reflux disease, or motility disorders like achalasia that disrupt the rhythmic movement of the esophagus.
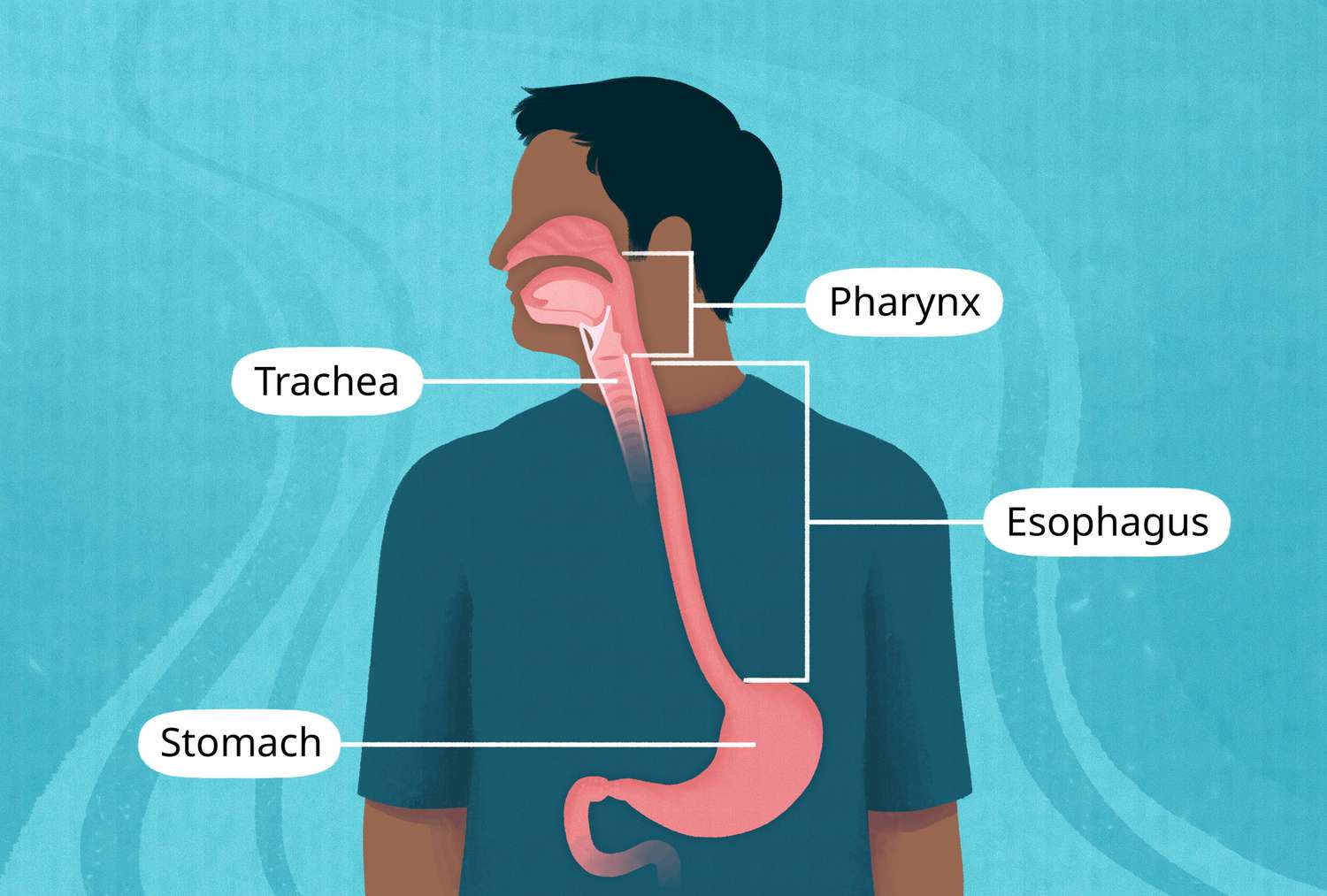
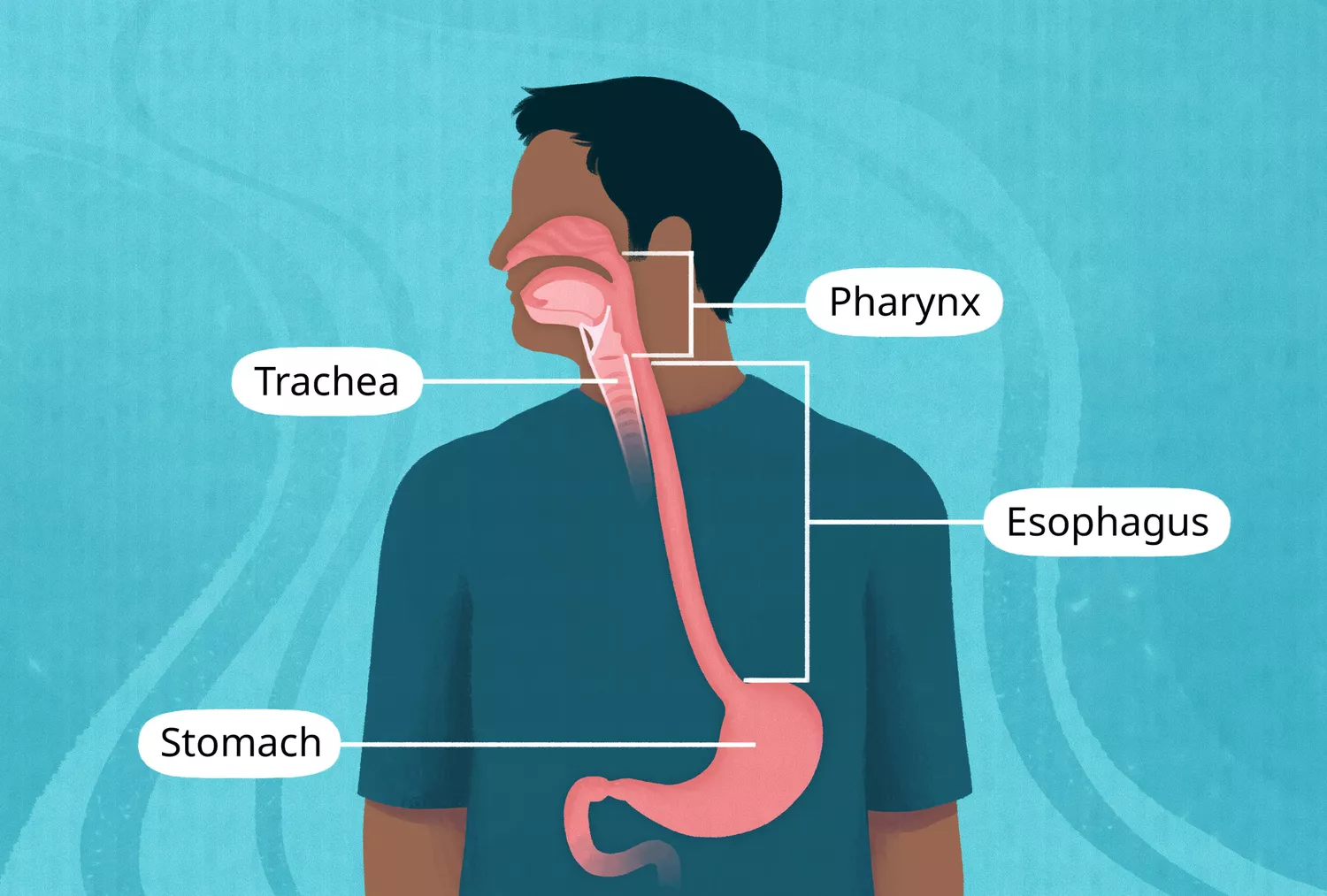
The Anatomy of a Swallow: Understanding the Four Layers
To understand how esophageal anatomy affects swallowing function, one must look closely at the sophisticated structure of the esophageal wall. This tube is not merely a passive pipe but a complex organ designed to transport a food bolus from the pharynx to the stomach through coordinated contractions known as peristalsis.
The innermost layer is the mucosa, which provides a protective lining and secretes mucus to ease the passage of food. Beneath the mucosa lies the submucosa, a layer of dense connective tissue containing blood vessels, nerves, and glands. The third layer, the muscularis propria, is responsible for the actual movement of food. Interestingly, the muscular composition of the human esophagus is not uniform. It transitions from striated muscle in the proximal third to smooth muscle in the distal third. This transition allows for the voluntary initiation of a swallow to give way to involuntary, rhythmic transport. Finally, the adventitia is the outermost layer of fibrous tissue that anchors the esophagus to surrounding structures in the chest.
When any of these layers are compromised, the esophageal anatomy and swallowing function are disrupted. For instance, scarring in the mucosa can lead to an esophageal stricture, narrowing the path for food. Disorders affecting the nerves within the muscularis propria can lead to achalasia, where the lower esophageal sphincter fails to relax, preventing food from entering the stomach.
Identifying the Origin: Oropharyngeal vs. Esophageal Dysphagia
Recognizing signs of swallowing disorders requires distinguishing where the problem begins. Clinicians categorize dysphagia into two primary types based on the location of the dysfunction: oropharyngeal and esophageal.
Oropharyngeal dysphagia is often neurological in origin, commonly seen after a stroke or in patients with Parkinson’s disease. In these cases, the patient struggles to move food from the mouth into the upper esophagus. You might notice coughing, gagging, or a sensation of food "going down the wrong pipe" immediately upon trying to swallow.
In contrast, signs of esophageal dysphagia vs oropharyngeal dysphagia involve a delay. The patient can usually initiate the swallow without trouble, but the food feels like it gets stuck in the chest or at the base of the throat a few seconds later. This sensation is often accompanied by pressure or even pain, known as odynophagia. Some patients may also describe a globus sensation, which is the feeling of a lump in the throat that is unrelated to the actual act of eating.
| Feature | Oropharyngeal Dysphagia | Esophageal Dysphagia |
|---|---|---|
| Primary Sensation | Difficulty initiating the swallow | Food feels "stuck" in the chest or mid-throat |
| Timing | Immediate (within 1 second) | Delayed (seconds after the swallow) |
| Associated Symptoms | Nasal regurgitation, coughing, choking | Heartburn, chest pressure, weight loss |
| Common Causes | Stroke, ALS, Myasthenia Gravis | GERD, Achalasia, Esophageal stricture |
Common Causes: From GERD to Achalasia
There are several underlying reasons why a person might experience dysphagia swallowing difficulty. Most causes fall into three categories: structural, inflammatory, and motility-related.
Gastroesophageal reflux disease is one of the most frequent culprits. Chronic exposure to stomach acid can cause inflammation, known as esophagitis, which may lead to the formation of an esophageal stricture. This narrowing of the esophagus makes it physically difficult for solid foods to pass. In some cases, a hiatal hernia can also contribute to reflux and subsequent swallowing problems.
Motility disorders represent a failure of the esophagus to coordinate its movements. In achalasia, the nerves in the esophagus are damaged, leading to the loss of peristalsis and the failure of the lower esophageal sphincter to open. This results in food sitting in the esophagus for extended periods, often leading to regurgitation of undigested food. Other conditions, such as diffuse esophageal spasm, can cause uncoordinated, high-pressure contractions that result in chest pain and intermittent swallowing difficulty.
The Diagnostic Path: What to Expect
If you are experiencing persistent trouble, the diagnostic steps for esophageal dysphagia usually begin with a referral to a gastroenterologist. The process is designed to rule out malignancies and identify the specific functional or structural abnormality.
One of the first tests often recommended is an upper endoscopy. During this procedure, a doctor inserts a thin, flexible tube equipped with a camera through the mouth and into the esophagus. This allows for a direct visual inspection of the mucosa and the ability to take biopsies if inflammation or an esophageal stricture is detected.
For a better understanding of the structural flow, you may be asked to undergo a barium swallow test. When preparing for a barium swallow test for dysphagia, you will be asked to drink a thick, chalky liquid containing barium. As you swallow, X-rays are taken to track the liquid's movement. This test is excellent for identifying narrowings, tumors, or problems with the lower esophageal sphincter that might not be as obvious during an endoscopy.
Finally, if a motility disorder is suspected, esophageal manometry is performed. This involves passing a thin, pressure-sensitive tube through the nose and into the esophagus. As the patient takes small sips of water, the tube measures the pressure and coordination of the esophageal muscles during bolus transport. This is the definitive test for diagnosing conditions like achalasia.
Management Strategies: Rehabilitative and Compensatory
Managing dysphagia involves a multidisciplinary approach tailored to the underlying cause. Strategies generally fall into two categories: rehabilitative (fixing the problem) and compensatory (adapting to the problem).
Rehabilitative treatments might include medical procedures such as esophageal dilation, where a balloon is used to stretch an esophageal stricture. For achalasia, surgery or Botox injections into the lower esophageal sphincter may be required. However, for many, the focus is on long-term management through lifestyle and dietary changes.
Modifying food consistency for safe swallowing at home is a critical compensatory strategy. Many patients find success using the International Dysphagia Diet Standardisation Initiative (IDDSI) framework, which categorizes foods from liquid to solid on a numbered scale. Using liquid thickeners can help prevent fluids from moving too quickly into the airway.
Additionally, swallowing exercises for adults with esophageal disorders can improve muscle strength and coordination. These exercises, often guided by a speech-language pathologist, help patients learn new techniques to clear the bolus transport more effectively and protect the airway.
Complications and When to See a Doctor
Ignoring dysphagia swallowing difficulty can lead to serious health complications. Beyond the immediate discomfort, chronic swallowing problems can result in malnutrition and dehydration because the individual may avoid eating or drinking to bypass the pain.
The most dangerous complication, however, is aspiration. This occurs when food, liquid, or saliva enters the lungs instead of the stomach. Recognizing signs of aspiration pneumonia from dysphagia is vital for early intervention. Warning signs include a persistent cough after eating, a "wet" or gurgly sounding voice, recurring chest infections, and unexplained fever.
If you find that food is consistently getting stuck, or if you experience unintended weight loss and chest pain during meals, it is time to consult a healthcare professional. Early diagnosis not only improves the quality of life but also prevents the long-term damage associated with chronic reflux and aspiration.
FAQ
What are the primary causes of swallowing difficulty?
Swallowing difficulty can stem from structural issues like an esophageal stricture or hiatal hernia, inflammatory conditions such as gastroesophageal reflux disease, or motility disorders like achalasia. Neurological conditions like stroke or Parkinson’s disease can also affect the coordination required to swallow.
What is the difference between oropharyngeal and esophageal dysphagia?
Oropharyngeal dysphagia involves difficulty starting the swallow and moving food from the mouth to the throat, often causing immediate coughing or choking. Esophageal dysphagia is the sensation of food getting stuck in the chest or lower throat several seconds after the swallow has been initiated.
How do doctors diagnose the cause of dysphagia?
Diagnosis usually involves a combination of medical history review and specialized tests. Common tools include an upper endoscopy to visualize the esophageal lining, a barium swallow test to see the structure of the tube via X-ray, and esophageal manometry to measure muscle pressure and coordination.
What are the early warning signs of dysphagia?
Early signs include having to cut food into very small pieces, needing extra liquid to wash food down, a persistent globus sensation (lump in the throat), or frequent heartburn. Pain during swallowing and a coughing fit during or after meals are also significant red flags.
Which foods should be avoided when you have trouble swallowing?
Individuals with dysphagia should generally avoid dry, crumbly foods like crackers, stringy meats like steak, and sticky substances like peanut butter. Many patients find that modifying food consistency for safe swallowing at home by pureeing solids or using thickeners for liquids makes eating much safer.





